Article Text

Abstract
Please confirm that an ethics committee approval has been applied for or granted: Yes: I’m uploading the Ethics Committee Approval as a PDF file with this abstract submission
Background and Aims Surgical correction of adolescent idiopathic scoliosis (AIS) requires high doses of opioids, traditionally via intravenous patient-controlled analgesia (IVPCA). An ERAS protocol was implemented at our institution to stop routine use of IVPCA, to be replaced with either intrathecal morphine injection or enteral methadone, and transition to enteral analgesia by morning after surgery.
Methods With REB approval, chart review was conducted of all patients who underwent surgical correction for AIS before and after protocol implementation, to compare outcomes and feasibility of managing pain with the ERAS protocol.
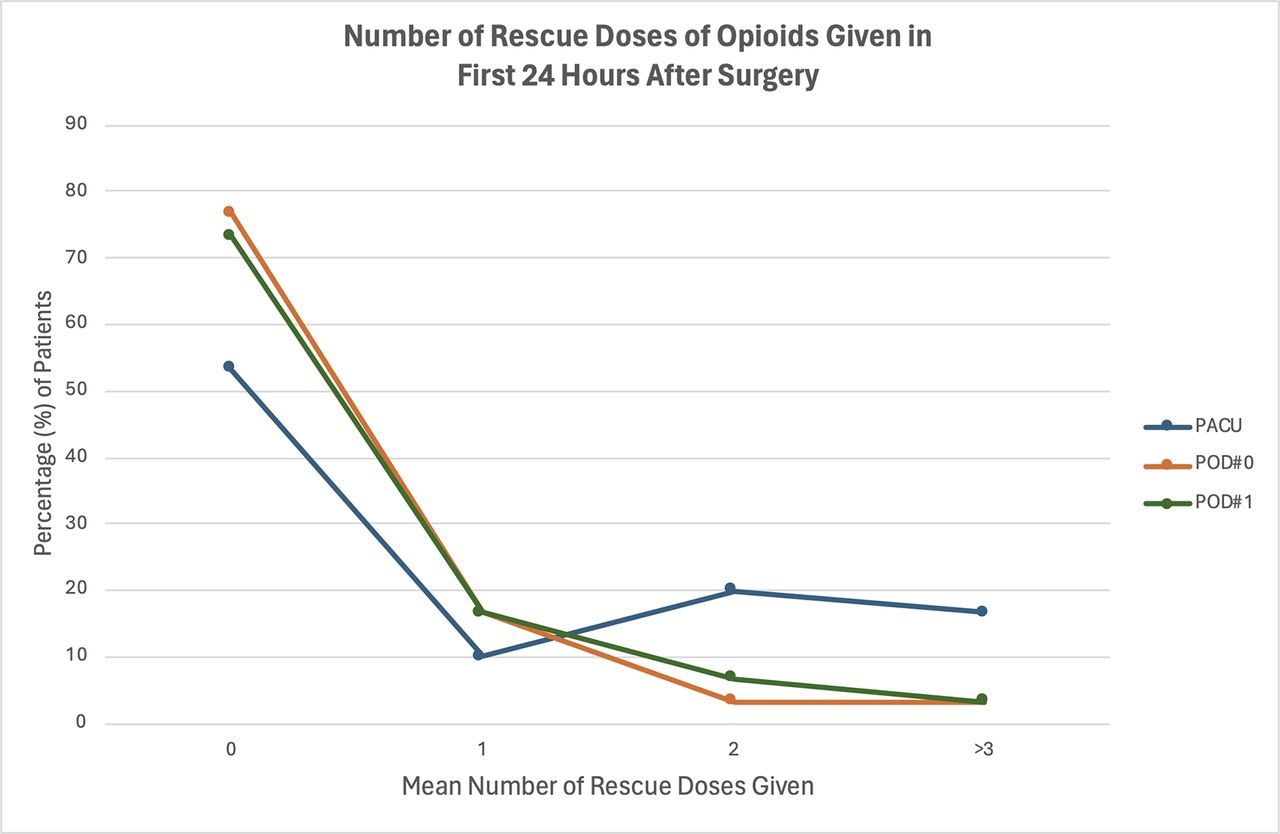
Results 62 patients were included, 32 receiving IVPCA and 30 in the ERAS pathway. No significant difference between groups by age, gender or BMI. Majority of patients in the ERAS pathway did not require rescue doses of opioids in the recovery room (53.3%), POD 0 (76.7%) or POD 1 (73.3%). There were statistically significant differences in pain scores between the two groups, with the IVPCA group having higher pain scores at 0 hours (p=0.002), ERAS group having higher pain scores at 24 hours (p=0.02) and 36 hours (0.01), with no difference in pain scores between groups at 12 hours (p=0.12). Length of stay in ERAS pathway (mean 3.16 days) versus IVPCA (2.83 days) pathway were not statistically significantly different (p=0.07).
Demographics and clinical characteristics between ERAS pathway and IVPCA groups
Differences in pain scores between ERAS Pathway and IVPCA patients

{kind=link}
Number of rescue doses of opioids given in 1st twenty four hours after surgery
Conclusions Analgesia after AIS repair can be successfully achieved without IVPCA, with intrathecal morphine or methadone, to allow for increased mobility, reduced use of resources and decreased reliance on intravenous medications. More judicious use of enteral rescue doses should be incorporated to further improve pain management.