Article Text

Abstract
Introduction The Microsoft HoloLens is a head-mounted mixed reality device, which allows for overlaying hologram-like computer-generated elements onto the real world. This technology can be combined with preprocedural ultrasound during thoracic epidural placement to create a visual of the ideal needle angulation and trajectory in the users’ field of view. This could result in a technically easier and potentially safer alternative to traditional blind landmark techniques.
Methods Patients were randomly assigned to one of two groups: (1) HoloLens-assisted thoracic epidural technique (intervention—group H) or (2) traditional thoracic epidural technique (control—group C). The primary outcome was needling time (defined as skin puncture to insertion of epidural catheter) during the procedure. The secondary outcomes were number of needle punctures, number of needle movements, number of bone contacts, and epidural failure. Procedural pain and recovery room pain levels were also evaluated.
Results Eighty-three patients were included in this study. The primary outcome of procedure time was reduced in the HoloLens group compared with control (4.5 min vs 7.3 min, p=0.02, 95% CI), as was the number of needle movements required (7.2 vs 14.4, p=0.01), respectively. There was no difference in intraprocedure or postprocedure pain, bone contacts, or total number of needle punctures. Three patients in the control group experienced epidural failure versus one patient in the HoloLens group.
Conclusions This study shows that thoracic epidural placement may be facilitated by using a guidance hologram and may be more technically efficient.
Trial registration number NCT04028284.
- Injections, Spinal
- Methods
- Pain Management
Data availability statement
Data are available on reasonable request. Not applicable.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Studies using phantoms have suggested a mixed reality headset-based technique may aid in accessing the neuraxial space.
WHAT THIS STUDY ADDS
This study suggests that thoracic epidural placement for major abdominal surgery using a mixed reality technique required less time and fewer needle movements compared with traditional techniques.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Mixed reality-based techniques using a guidance hologram may be preferred for thoracic epidural placement, considering it may be more technically efficient compared with controls.
Introduction
Neuraxial anesthesia and interventional pain techniques (spinal and epidural) have traditionally been a ‘blind’, landmark-based technique. The subarachnoid or epidural space is identified via anatomical landmarks, relying on operator feel and skill. However, this is highly influenced by patient body habitus where obese patients or those with anatomical variations can prove to be quite challenging.1 2 Neuraxial anesthesia is not a benign procedure as multiple attempts of the needle can be anxiety provoking, cause patient discomfort, and also may lead to increased risk for spinal/epidural hematomas, infection, dural puncture headaches, and nerve injury.3
The use of ultrasound (US) has become standard of care for peripheral nerve blocks as it allows for real-time observation of the needle position in relation to target structures achieving higher rates of success, fewer complications, reducing patient discomfort, and quicker procedural times.4 Due to technical challenges,5 the common technique for US use in neuraxial anesthesia is to provide preprocedure landmarks so the operator has a prediction for the placement of the needle tip, trajectory and depth before actual needle insertion.5 6
Multiple reviews have been published demonstrating preprocedure US reduces procedure time, number of needle passes, needle contact with bone, and other complications in the midline approach to the lumbar spine compared with traditional placement techniques based on operator feel.6 7 The common technique for thoracic epidurals perioperatively is a ‘paramedian’ approach owing to anatomical differences in the thoracic spine. This involves intentionally contacting lamina with the needle and continuously adjusting in a cephalad/midline direction while advancing until loss of resistance is achieved, which can prove to be quite challenging.8 Trials using preprocedural US for thoracic epidural placement are limited and have not conclusively reduced procedure time or number of needle redirections.9–11 Hence, US is yet to be commonly adopted as an approach for thoracic epidurals.
Mixed reality (MR) head mounted displays allow for positionally stable virtual data to be projected into a user’s visual field, similar to a hologram.12 Medical applications have included education, remote consultation, preoperative surgical planning, and surgical/procedural navigation, typically on an experimental level.13 Emerging evidence demonstrates potential benefits including reduced procedure time and greater accuracy when applied to phantom procedure models.14 15 We have previously described an MR-based needle guidance system using the Microsoft HoloLens headset (Microsoft, Redmond, Washington, USA), which allows a representation of the ideal needle angulation identified during a preprocedural US to serve as a visual aid during thoracic epidural placement.16 To our knowledge, there are no randomized trials to date in clinical settings relating to MR-guided neuraxial procedures. This knowledge gap warrants further comparative studies.
This is the first randomized trial to compare the effectiveness of traditional and MR-guided neuraxial techniques in a real clinical setting. We hypothesized using the HoloLens system would improve the approach, difficulty, and time required for thoracic epidural placement. The primary outcome was the procedure time. Secondary outcomes included number of needle punctures, number of needle movements, number of bone contacts, epidural failure, procedural pain, and recovery room pain levels.
Methods
Trial design
Patients were enrolled from January 18, 2019 to February 19, 2021. This study was first registered and released September 6, 2018 at ClinicalTrials.gov identifier NCT04028284. There was a dialog with reviewers which resulted in a rereview and final approval of the entry in July 2019 without modifications to trial procedures or conduct (online supplemental file 1).
Supplemental material
Participants
The study was approved under a verbal assent consent model for patients who had provided consent to a thoracic epidural for postoperative analgesia. We reasoned the intervention did not entail any additional significant risk to the patient, as procedures in both study arms were ultimately guided by the same tactile feedback such as loss of resistance. Only patients who met inclusion criteria were approached for participation in this study before their procedure. They were informed about the purpose, procedures, benefits/risks, and were given enough time to read a lay study summary and ask questions about the study. The study research team ensured that the participants knew their participation was voluntary and they had the right to withdraw from the study/collected data at any time. Informed consent was obtained from the anesthesiologists performing the epidural procedure as they were subjects and randomized. Patients undergoing abdominal surgery with a planned thoracic epidural catheter participated in this study.
Patient inclusion criteria were ≥18 years old and American Society of Anesthesiology Physical Status I to IV undergoing any thoracic or upper abdominal elective surgery with planned thoracic epidural analgesia. Exclusion criteria were contraindications to epidural catheter, pregnancy, preexisting coagulopathy, localized infection, and known allergy to local anesthetics.
Randomization, allocation, blinding
In this study four staff anesthesiologists experienced in regional anesthesia and in preprocedure US-guided epidural techniques participated. All anesthesiologists completed a training session where they practiced the MR technique on thoracic spine phantoms until they were comfortable with the procedure and deemed competent by study staff.16 A fifth anesthesiologist participated on a pilot basis during the training phase only as they departed our institution. At each epidural insertion event, the four subjects were randomized (1:1) to landmark or preprocedure US-guided thoracic epidural technique, as per operator preference (group C), or MR guidance (group H). The randomization sequence was computer generated by non-clinical study staff with allocations placed in sealed, sequentially numbered envelopes, opened only at the time of epidural placement to maintain allocation concealment. The epidural level targeted was determined by the procedural anesthesiologist based on the planned surgical incision.
Study procedure and data collection
In group C (control), the staff anesthesiologist followed the traditional technique for landmark or preprocedure US-guided thoracic epidural insertion (as per their preference). Briefly, the anesthesiologist used landmarks or the US to identify and mark the appropriate spot on the skin for insertion of the epidural needle. Local infiltration was with 1–5 mL of 2% lidocaine solution with a 25G needle, followed by 2 min of waiting. The US probe was then placed at rest and the anesthesiologist proceeded with thoracic epidural needle insertion following standard techniques.
In group H, the staff anesthesiologist used the HoloLens system in combination with the US to obtain a hologram image of the trajectory toward the epidural space, thereby mitigating the need to walk off the lamina. The operator performs the procedure while wearing the HoloLens headset, which minimally interferes with procedure ergonomics and visibility. A preprocedural, non-sterile US scan of the spine was performed with the prepared tracking marker attached to the transducer (figure 1). The posterior complex is identified and placed in the middle of the US screen. The angulation of the US transducer is then registered by the headset detecting the position of the US transducer marker, and a hologram is projected into the user’s workspace, which replicates the needle path through the middle of the transducer (figure 1 inset) in a clear path from skin to posterior complex. The central axis of the US transducer is represented by a holographic orange line (10 mm length, 2 mm diameter).

The user performs a preprocedural ultrasound, allowing the headset to detect the position of the ultrasound transducer and subsequently generate a spatially stable hologram. The inset shows the operator’s mixed reality view displaying a holographic guidance graphic which recreates the angulation of the transducer (orange line along the central axis of the ultrasound transducer).
The transducer is removed from the field, and its center point is marked on the skin in the usual fashion. The spatially stable hologram representing the ideal needle path remains projected into the user’s visual field although the hologram does not provide any information on the desired needle depth nor does it register the needle’s position in the user’s visual frame. Typical sterile prepping and draping and local anesthetic injection do not disrupt the position of the needle path hologram. Operators may then use this hologram to precisely align the needle angulation with the holographic projection in three dimensions from the marked skin entry point. The MR system served as a guide to needle angulation only, with the skin insertion site being noted relative to the US by standard techniques. The Tuohy needle was then inserted by following the MR/holographic trajectory overlaid on the patient’s back.
We have previously published additional figures of this MR technique and video performed on a phantom spine model.16
Outcomes
For the primary outcome, an independent observer documented the time to procedure completion starting at skin puncture to withdrawal of the Tuohy needle after successful catheter placement. We chose to use procedure time as this is the time period where patient morbidity might occur, and where patient anxiety might be greatest. Continuous secondary outcomes, the number of needle passes, needle skin punctures, and needle to bone contacts were also recorded by the trained observer. A “needle pass” was defined as any advancement of the needle along an unchanged trajectory. A “needle skin puncture” was defined as complete needle withdrawal from the skin and reinsertion at a new location. The anesthesiologist performing the procedure would indicate verbally to the independent observer when a needle to bone contact occurred. The observer also documented any signs of complications during the procedure such as paresthesia, dural punctures, as well as procedure failure rates.
A questionnaire regarding the patients’ level of discomfort during the procedure (on a scale of 0–10, with 0 being no pain/no discomfort and 10 being worst possible pain/extreme discomfort) was administered to the patient on completion of the epidural procedure, as well as in the recovery room after the surgical procedure. The ease of use and limitations of each technique were also evaluated using a questionnaire given to the regional anesthesiologist following each procedure.
Epidurals were managed intraoperatively by anesthesiologists not involved in the study with local anesthetic concentration and timing as per their standard of care. Epidural failure was defined as unexpected addition of intravenous patient controlled analgesia to the patient’s pain control regimen prior to discharge from the recovery room.
Sample size calculation
Based on historical data in the literature and from our own institution, mean thoracic epidural analgesia placement requires 10 min with an SD of 3 min. We considered a reduction in procedure time of 2 min (20% relative reduction) to be meaningful in the context of patient comfort and operating room efficiency. With a two-sided type I error rate of 5% and power 80%, 36 participants per group (72 total) were required; recruitment of 84 patients was planned to compensate for potential withdrawals.
Statistical analysis
The primary outcome, time to epidural placement, was analyzed as follows. Times were assessed for normality with the Shapiro-Wilk test. If normally distributed, data was analyzed with the independent samples t-test. If the assumption of normality was violated, the Mann-Whitney U test for non-parametric data was used. Secondary outcomes that were continuous in nature (number of skin punctures, number of needle passes, procedural pain) were analyzed in the same manner. For binary outcomes (parasthesias, dural puncture, success rate) the χ2 test (or Fisher’s exact when expected cell counts are less than 5) was used. Categorical variables are presented as frequency and percentages. Normally and nonnormally distributed variables were presented as the mean (SD) and the median (1st–3rd quartiles, (range)), respectively. All inferential testing will be two sided and a p<0.05 was considered significant for the primary outcome. To account for multiple comparisons, inferential testing for secondary outcomes was adjusted with the Holm-Bonferroni method.
Results
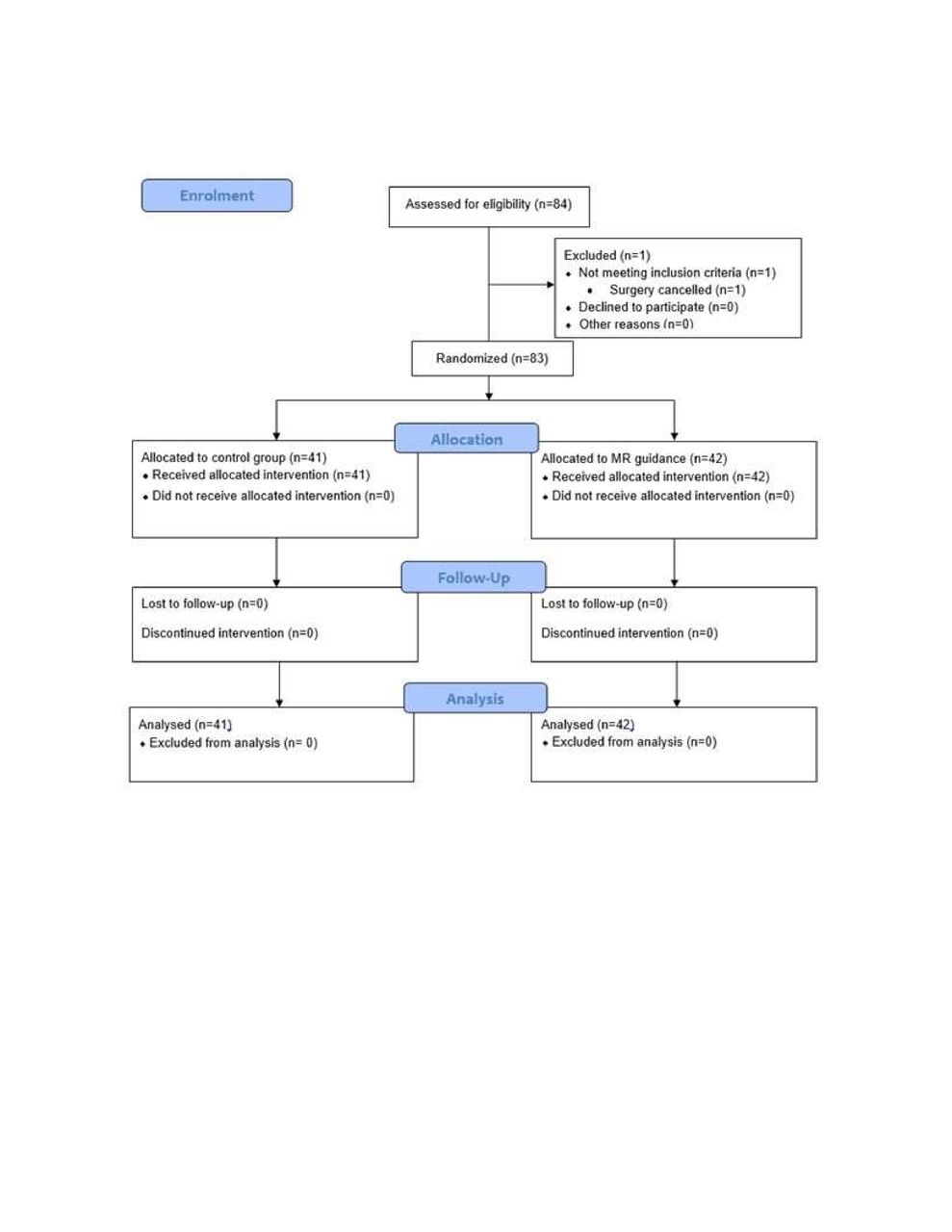
Randomization occurred for 83 epidural placement events. Forty-two were assigned to group C while 41 were assigned to group H. Figure 2 describes patient flow through the study.

{kind=link}
{kind=link}
Consolidated Standards of Reporting Trials diagram of patient flow through the study. MR, mixed reality.
Demographic data, including age, sex and surgery type were similar between the two groups (table 1).
Demographics
The primary outcome of procedure time was significantly reduced in the HoloLens group relative to control (4.5 min vs 7.3 min, p=0.02), as was the number of needle passes required (7.2 vs 14.4, p=0.01) (table 2). In a single patient in the control arm of the study, the anesthesiologist used a preprocedural US, all other controls used landmark technique only. There was no significant difference in intraprocedure or postprocedure pain, bone contacts or total number of needle punctures. Notably, while not significant, epidural administration failed in three participants in the control group, compared with zero participants in the HoloLens group (table 2). Registering the guidance hologram typically required 1–2 min during the anesthesiologist training phase of the study.
Outcomes
Discussion
To our knowledge, this is the first report of a randomized trial in a clinical setting of MR guidance with a head mounted display in the application of neuraxial anesthesia. Our study shows a head mounted display, HoloLens-assisted, US guidance system for thoracic epidural placement was safe, faster, and with fewer needle passes and movements compared with standard techniques.
While subjects in the holographic group endured shorter epidural procedures with fewer needle passes, they did not rate their pain during the procedure as less, or experience less rated pain in the recovery room (although our study was not powered to find these differences). There was no significant difference in epidural failure between the groups, although the holographic group had no failures and the control group had three. The most appropriate definition of epidural failure is of some discussion and this may have influenced this outcome.17 Besides the reduced number of needle passes, there were no other differences in the secondary outcomes.
Previous preclinical studies have hinted at potential advantages to applying MR or similar augmented reality (AR) systems to neuraxial procedures. In a system using an MR headset to access the neuraxial space in spine phantoms, Reinacher et al recently showed reduced procedure time, improved first pass success, and reduced needle angular deviation from the ideal.14 However, this system did not have the capability for an operator to determine and follow their own ideal needle path, instead relying on a predetermined one (which is not applicable to clinical practice). Similarly, a study using real-time AR visualization of needle tip position using a custom made US probe found increased success in accessing the epidural space in a phantom model.15 Our trial would suggest that these advantages seen in phantom studies is also applicable under real clinical conditions including anatomical variability and the potential for patient movement, at least with the system used in this study. More broadly, MR/AR systems have also shown promise in prototype systems for other image guided procedures such as the CT-guided biopsy of lung lesions18 and MRI-guided cadaveric perineural injections of the hypogastric plexus.19
Not all needle-guided procedures are amenable to real time US guidance, and our MR-guided technique may be a useful alternative in these scenarios by allowing the depiction of an ideal needle path as a guide. Our system may also be useful for alternate procedures such as peripheral nerve block in patients that cannot be easily positioned for live US techniques and in patient populations with potentially difficult anatomy.
This holographic technique may also be of use in teaching thoracic epidural anesthesia or assisting operators with less experience. Previous work has shown that needle visualization while training leads to improved learning performance,20 which may apply to this MR based system. Our participants, who were experienced regional anesthesiologists, experienced a technical benefit. The required training sessions were typically 10 min in length. It is possible this effect could be magnified in operators with less or more infrequent thoracic epidural insertion experience. Although we have not applied it in such a manner in this study, the HoloLens is capable of streaming video of the operator’s field of view and could be amenable to remote procedural coaching. Further research is warranted regarding this technology with respect to operators with less regional anesthesia experience or more patient groups known to present greater clinical challenges.
Implementing MR and AR systems in clinical roles may cause challenges with attentional blindness, maintaining procedural sterility, and visual distortions which we did not explicitly measure in our study.21 In addition, many MR/AR systems are expensive, the most recent version of the HoloLens currently retails for US$3500.22
There are several limitations to this study. We did not compare our MR-guided technique strictly to a landmark based technique; at our institution, some anesthesiologists have incorporated routine preprocedure US scans as standard of care, and therefore, we chose to not exclude this from the control arm of our study. The anesthesiologists involved in the study were all experienced in regional anesthesia, and the observed effects may not be generalizable to novices or those that perform thoracic epidurals with low frequency. While this did not occur during our study, the MR-guided technique would require a repeat US scan and registration of the needle path hologram should the patient have any significant movement while needling was underway. Also, the anesthesiologist who developed this technique and produced the related software was involved in training the remainder of the physicians involved in the study. Training will be essential in attaining competence in using this system.
Conclusions
This study has demonstrated that an MR guidance system using a head mounted display leads to increased procedural efficiency (eg, decreased procedure times and reduced needle movements), relative to traditional techniques. However, further study is needed to ensure that increased procedural efficiency with the HoloLens system translates to improved patient outcomes such as reductions in failure of complications.
Data availability statement
Data are available on reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This was a single-center, randomized, and controlled trial at Sunnybrook Health Sciences Centre, Toronto, ON; the study was initiated after approval by the Sunnybrook Research Institute Ethics Board (#291-2018).
Acknowledgments
We would like to acknowledge Eileen Wiegelmann for formatting the manuscript for submission.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JW and FA conceived the study. JW developed the software/equipment related to needle guidance. FA, CM, SC, PGM and OS participated in HoloLens device training, and system design guidance. JW and FA performed a literature search and were the major contributors in writing this manuscript. LK assisted with study coordination and data gathering. All authors edited the final version of the manuscript. All authors read and approved the final manuscript. JW is the guarantor of this manuscript.
Funding This work was supported by a grant from the Academic Health Sciences Centre Alternative Funding Plan, IFPOC (SHS-18-009).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.